Knee replacement Gold Coast
Knee replacement resurfaces the worn parts of an arthritic knee with artificial components, relieving pain and restoring movement. Dr Jason Tsung performs total and partial knee replacement using robotic-assisted planning, a functional alignment approach, and, for suitable patients, an anterolateral skin incision designed to reduce the numbness that commonly follows knee replacement. He has performed over 1,000 hip and knee replacements.
Written and reviewed by Dr Jason Tsung, FRACS (Orth) · Last reviewed June 2026
Who performs knee replacement on the Gold Coast?
Dr Jason Tsung performs total knee replacement, partial knee replacement and robotic-assisted knee replacement at Southern Gold Coast Orthopaedics in Tugun on the Gold Coast. Total knee replacement resurfaces the whole joint; partial (unicompartmental) knee replacement replaces a single worn compartment; and robotic knee replacement uses a CT-based plan to position the implant. Which option suits you depends on how the arthritis is spread across the knee, and Dr Tsung advises which fits at your consultation. He consults as an orthopaedic surgeon in Tugun and operates next door at John Flynn Private Hospital, followed by an enhanced recovery after surgery pathway. Individual results vary.

When is knee replacement considered?
Knee replacement is usually considered when arthritis pain no longer responds to non-surgical treatment, and when it interferes with walking, working, or sleep. It isn't the first step. Most knee arthritis is managed for a long time with physiotherapy, activity and weight management, and simple pain relief, and surgery comes into the picture only when those stop giving enough relief. If you haven't worked through those options yet, start with hip and knee arthritis management. The decision to operate is yours to make with your surgeon.
What happens during a knee replacement?
In knee replacement, the worn surfaces of the joint are removed and replaced with smooth metal and plastic components. A metal cap is fitted to the end of the thighbone, a metal plate with a plastic spacer is fitted to the top of the shinbone, and the back of the kneecap may be resurfaced. Only the worn surfaces are replaced, and the ligaments and muscles around the knee are kept in place so the joint moves naturally. The operation usually takes one to two hours, and most people stay in hospital for one to three days.
Total and partial knee replacement
In a total knee replacement, all the worn surfaces of the knee are resurfaced. If only one part of the knee is affected by arthritis, you may be suitable for a partial (unicompartmental) knee replacement, which replaces just that compartment and leaves the rest of the knee intact. Not everyone is suitable for a partial knee replacement; it depends on how the arthritis is distributed across the joint. Dr Tsung will advise which option fits your knee.
What is functional alignment?
No two knees are the same. The natural shape and alignment of the knee vary from person to person, and only about one in seven people have the neutral, straight-line alignment that older knee replacement techniques were built around.¹ Functional alignment positions the implant to suit your knee's own shape and ligament balance, rather than fitting every knee to a single textbook target, with as little release of the surrounding soft tissue as possible.
Robotic planning is what makes this practical and repeatable. Working from the CT-based plan, Dr Tsung checks the balance of the knee through its range of movement and adjusts the implant position before any bone is cut. A 2025 study found robotic functional alignment reached the planned alignment more accurately than conventional instruments.² A 2025 randomised trial reported that functional alignment needed far fewer soft-tissue releases than the traditional approach, and more patients said they would recommend the surgery, although overall scores were similar between the two groups at two years.³ Whether functional alignment makes a knee replacement last longer is not yet known, and longer-term registry data will answer that over the coming years. More on functional alignment.
The anterolateral skin incision
The most common complaint after knee replacement is a patch of numb skin on the front of the knee. It happens because a small nerve, the infrapatellar branch of the saphenous nerve, crosses the front of the knee just below the kneecap, and a traditional straight cut down the middle often divides it.⁴ The numbness isn't dangerous, but it can be bothersome and can make kneeling uncomfortable.
For suitable patients, Dr Tsung uses an anterolateral skin incision, a curved cut placed slightly to the outer side of the kneecap. Only the position of the skin cut changes. Once through the skin, the deeper part of the operation is the same as a standard knee replacement.⁴ Placing the cut to the side is designed to go around the nerve rather than through it.
A 2026 meta-analysis of eight randomised trials, involving 609 patients, found the anterolateral incision lowered the risk of numbness at one year by about 64% and reduced the size of the numb patch by roughly two-thirds, with no difference in knee movement, pain relief or satisfaction.⁴,⁵ In a study of patients who had both knees replaced, one with each type of incision, patients consistently preferred the knee with the anterolateral incision, and recovery of sensation was better over the first year.⁶
How is robotic assistance used in knee replacement?
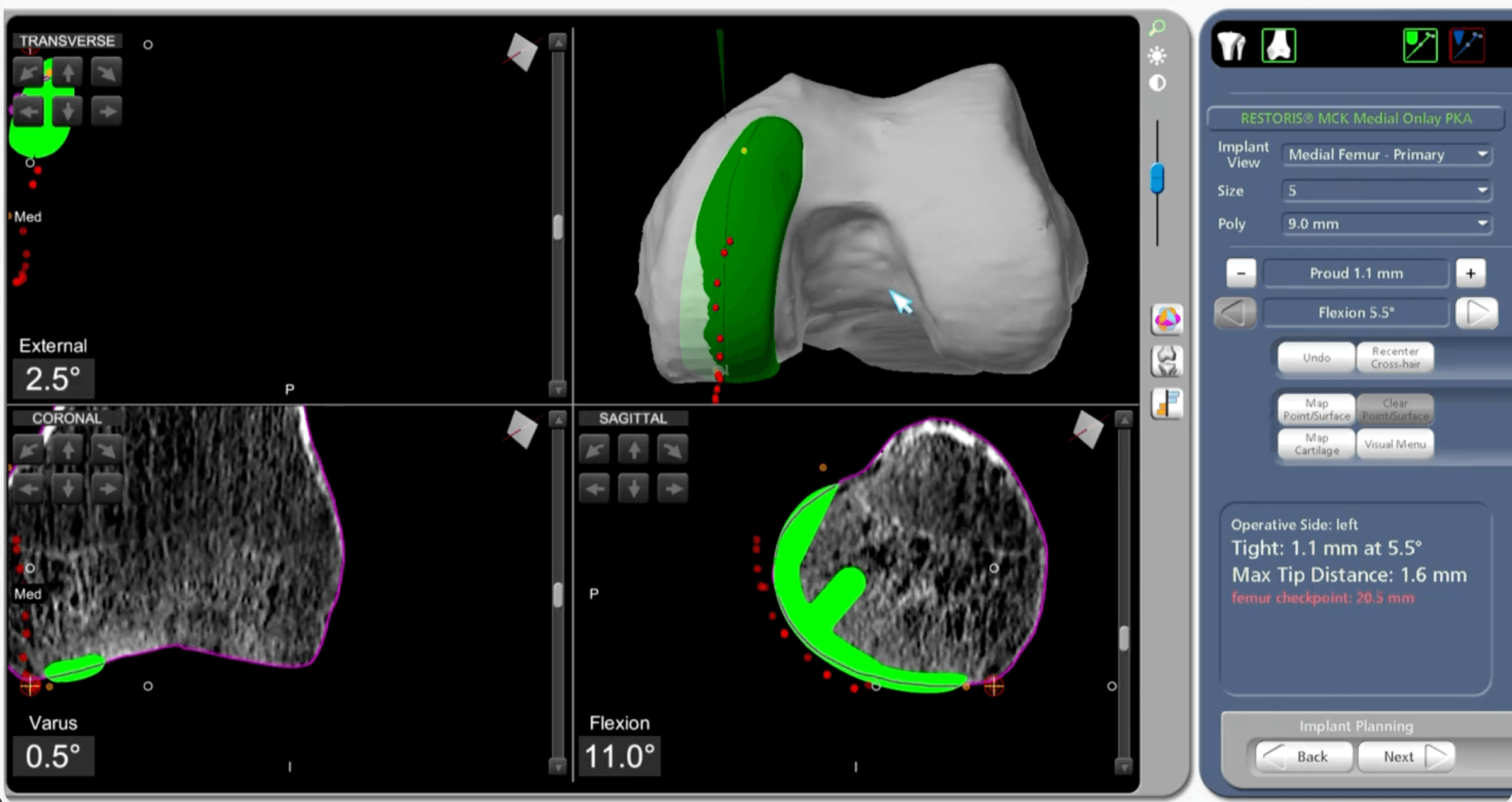
Dr Tsung uses the Stryker Mako robotic-arm system to plan and position the implant from a CT scan of your knee. In the knee, this delivers the functional alignment plan and places the implant with fewer alignment outliers than manual technique.⁷ More on robotic knee replacement and robotic-assisted joint replacement.
Enhanced recovery, or rapid recovery
Dr Tsung follows an enhanced recovery after surgery (ERAS) pathway for knee replacement, sometimes called rapid recovery. This combines modern pain control that reduces the need for strong painkillers, measures to limit bleeding and prevent blood clots, and getting you up and moving on the day of surgery. The aim is a smoother recovery and a shorter hospital stay, and individual recovery varies. More on enhanced recovery after surgery.
What are the risks of knee replacement?
Knee replacement relieves pain and improves mobility for most people, and serious complications are uncommon. As with any major surgery, risks exist and are worth understanding. They include infection, blood clots in the leg or lung, stiffness, a patch of numbness near the scar, loosening or wear of the implant over many years, nerve injury, fracture, and ongoing pain in a small number of cases. Knee replacement is also good at relieving pain but the new knee will not feel identical to a natural knee, and activities such as running and jumping are generally not recommended. Dr Tsung will go through the risks that apply to your situation at your consultation. Individual results vary.
What is recovery like?
Most people are up and walking with aids on the day of surgery or the day after, move from crutches to a stick over the following weeks, and bend the knee to around 90 degrees by the end of the second week. The first two weeks are usually the most uncomfortable part. Most people return to driving and desk work within several weeks, and full recovery continues over six to twelve months. Modern knee replacements are durable, and Australian registry data show that around 95% are still functioning at ten years.⁸ A more detailed week-by-week guide is on knee replacement recovery, and you can read more about implant lifespan on how long a knee replacement lasts.
Common questions
Who performs knee replacement on the Gold Coast?
Dr Jason Tsung performs total, partial and robotic-assisted knee replacement at Southern Gold Coast Orthopaedics in Tugun on the southern Gold Coast. He consults as an orthopaedic surgeon in Tugun and operates at John Flynn Private Hospital next door. Which option suits you depends on how the arthritis is spread across the knee, and Dr Tsung advises which fits at your consultation. Individual results vary.
Should I have a total or partial knee replacement?
Whether you have a total or partial knee replacement depends on how much of the knee is affected by arthritis. A total knee replacement resurfaces all the worn surfaces, while a partial (unicompartmental) replacement replaces just one worn compartment and leaves the rest of the knee intact. Not everyone is suitable for a partial replacement; it depends on how the arthritis is spread across the joint and the state of your ligaments. Dr Tsung advises which fits your knee. More on total versus partial knee replacement.
Will I be able to kneel after a knee replacement?
Many people can kneel after a knee replacement, though it often feels uncomfortable rather than impossible. A common reason is a patch of numb skin on the front of the knee, caused by a small nerve that a traditional cut can divide. For suitable patients Dr Tsung uses an anterolateral skin incision designed to go around that nerve and reduce the numbness. Kneeling does not damage the implant, and comfort often improves as recovery continues.
How long is recovery after a knee replacement?
Most people are up and walking with aids on the day of surgery or the day after, and the first two weeks are usually the most uncomfortable part. We follow an enhanced recovery pathway to get you moving early. By the end of the second week many people can bend the knee to around 90 degrees, and most return to driving and desk work within several weeks. Full recovery continues over six to twelve months, and there's a guide on knee replacement recovery.
What does functional alignment change?
Functional alignment positions the implant to suit your knee's own shape and ligament balance, rather than fitting every knee to one textbook target. Only about one in seven people have the neutral, straight-line alignment that older techniques were built around. Robotic planning makes the approach repeatable, and recent randomised trials report fewer soft-tissue releases with functional alignment. Whether it makes a knee replacement last longer is not yet known, and longer-term registry data will answer that.
What are the main risks of a knee replacement?
Knee replacement relieves pain and improves mobility for most people, and serious complications are uncommon, but like any major surgery it carries risks. These include infection, blood clots in the leg or lung, stiffness, a numb patch near the scar, loosening or wear over many years, nerve injury and fracture, with ongoing pain in a small number of cases. A replaced knee also won't feel identical to a natural knee, and running and jumping are generally not recommended. Dr Tsung discusses the risks that apply to you, and results vary.
How long does a knee replacement last?
Most modern knee replacements are still working well ten years after surgery, and many last considerably longer. Australian registry data show that around 95% of knee replacements are still functioning at ten years. How long any individual knee lasts depends on factors like your age, weight, activity level and the implant used, and a small number need revision surgery over time. More on how long a knee replacement lasts.
Book or refer
To see Dr Tsung you’ll need a referral from your GP or another specialist. Call reception on (07) 5676 9930 to book your first appointment, or email hello@sgco.au. New patients can pre-register online before the visit; the form prepares your records and does not book an appointment. For costs, see fees and health funds.
References
- MacDessi SJ, et al. Coronal Plane Alignment of the Knee (CPAK) classification. Bone & Joint Open. 2021.
- Sava M, et al. Improved accuracy of functional alignment restoration with robotic-assisted total knee arthroplasty. Die Orthopädie. 2025.
- Young SW, et al. The John N. Insall Award: functional versus mechanical alignment in TKA, a randomised controlled trial. Journal of Arthroplasty. 2025.
- Laffosse JM, et al. Anterolateral skin incision in total knee arthroplasty: a randomised controlled trial. 2011.
- Mostafa AAS, et al. Effect of anterolateral skin incision on numbness after total knee arthroplasty: a meta-analysis. 2026.
- Maniar RN, et al. Anterolateral versus midline incision in bilateral total knee arthroplasty: a prospective randomised study. 2017.
- Ruangsomboon P, et al. Robotic-assisted versus conventional total knee arthroplasty: a meta-analysis of randomised controlled trials. Annals of Medicine and Surgery. 2025.
- Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR). Hip, Knee & Shoulder Arthroplasty: 2025 Annual Report. Adelaide: AOA; 2025.