Robotic-assisted joint replacement Gold Coast
Dr Jason Tsung uses the Stryker Mako robotic-arm system to plan and perform hip and knee replacement, and has done so since 2016. The robot doesn’t perform the surgery. Dr Tsung does. It’s a guidance tool that helps him position your new joint accurately, working from a plan built around your own anatomy. Across his career, Dr Tsung has performed over 1,000 hip and knee replacements.
Written and reviewed by Dr Jason Tsung, FRACS (Orth) · Last reviewed June 2026
Who offers robotic knee replacement on the Gold Coast?
Dr Jason Tsung performs Mako robotic-assisted knee replacement on the Gold Coast, covering total knee replacement and partial (unicompartmental) knee replacement, at John Flynn Private Hospital in Tugun. Robotic planning works from a CT scan of your knee and is used to deliver the functional alignment plan. More on robotic knee replacement, knee replacement and partial knee replacement. Robotic assistance is a planning and guidance tool rather than a guarantee of a particular result, and individual results vary.

What is robotic-assisted joint replacement?
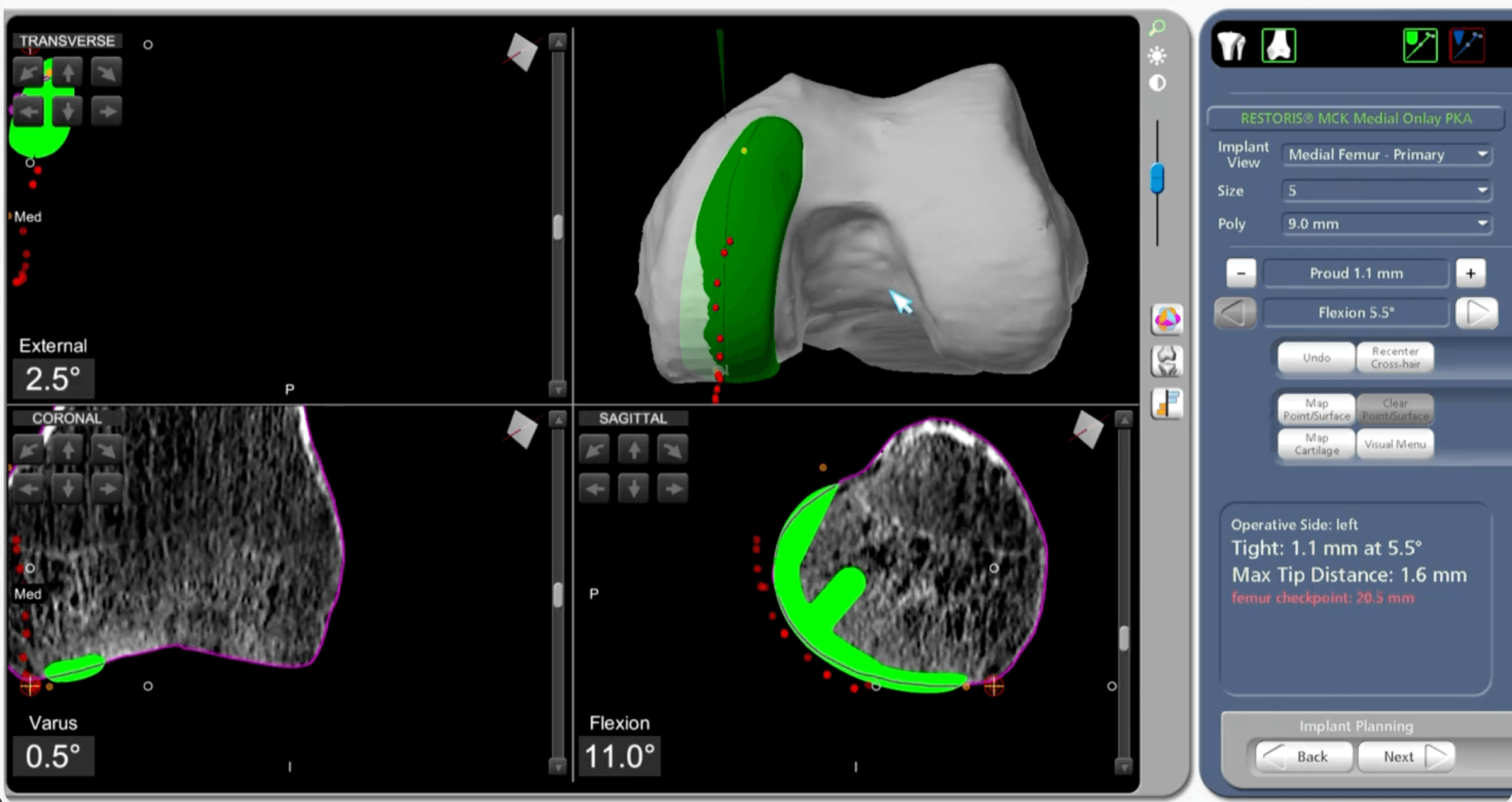
Robotic-assisted joint replacement is conventional joint replacement carried out with the help of a robotic-arm system, with the surgeon in control throughout. With the Mako system, a CT scan taken before surgery is turned into a 3D model of your joint. The implant is planned onto that model, and during the operation the robotic arm helps Dr Tsung follow the plan precisely.
How does the Mako system work?
The system supports four steps:
- Plan. A low-dose CT scan, taken a week or two before surgery, becomes a 3D model of your hip or knee. The size, position and angle of your implant are mapped onto it.
- Check and balance. In theatre, Dr Tsung matches the bone to the plan and checks the soft tissues. If anything needs adjusting, the plan is changed before any bone is cut.
- Prepare the bone. A boundary set in the plan keeps the instrument inside the intended area, and the arm resists if it moves outside it. The robot never moves on its own. It limits where the surgeon can go.
- Reassess. Trial components go in, the balance is checked again, and final adjustments are made if needed.
Does robotic assistance lead to better results?
The best-proven benefit of robotic assistance is precision: placing the implant more accurately and more consistently than manual technique. Some benefits patients can feel are also reported, mostly in early recovery. It also matters what robotic surgery hasn't been shown to do.
Precision: strong, consistent evidence. Across hip and knee replacement, robotic assistance places implants more accurately, with fewer ending up outside the planned alignment. In knee replacement, pooled randomised trials found it reduced the chance of an implant falling outside the target alignment by about two-thirds.¹ In hip replacement, the socket was placed in the position surgeons aim for (the "safe zone") in around 95% of robotic cases, compared with roughly 66% using conventional instruments.²
Early recovery: modest, mostly short-term. Some studies report that, in the first days and weeks, patients having robotic knee replacement may have less pain, use fewer opioid painkillers, and go home a little sooner than with manual surgery.³,⁴ These differences are real but modest, and they tend to even out over the following months.
Long-term results: similar to conventional surgery. Some pooled studies suggest modestly better knee function in the first months to a year,⁵ and a randomised trial found greater improvement in knee pain over the first year, though not in overall function or quality of life.⁶ Beyond that, national joint replacement registries and recent reviews have not shown that robotic assistance makes a hip or knee replacement last longer, or need fewer revisions, than well-performed conventional surgery.⁷,⁸ Precision is the proven benefit. The current evidence does not show a clear difference in the long-term result.
Robotic hip, knee and partial knee replacement
Dr Tsung uses the Mako system for hip replacement, total knee replacement, and partial (unicompartmental) knee replacement. The benefit is a little different for each.
Hip replacement. The system helps position the socket accurately within the target zone, the area linked to a lower chance of the hip dislocating. Some large studies report lower dislocation rates when the socket is well placed.²,⁹ Robotic planning can be combined with the minimally invasive direct superior approach Dr Tsung uses for many hip replacements. More on hip replacement and robotic hip replacement.
Knee replacement. In the knee, the Mako system delivers a functional alignment plan, positioning the implant to suit your knee's own shape and ligament balance, with fewer alignment outliers than manual technique. More on knee replacement and robotic knee replacement.
Partial (unicompartmental) knee replacement. Partial knee replacement is technically demanding and less forgiving of small positioning errors, which is where robotic precision may matter most. A 2026 review of nearly 9,000 partial knee replacements found fewer alignment outliers with robotic assistance.¹⁰ Registry and pooled data suggest robotic-assisted partial knee replacement may have lower revision rates than many conventional partial-knee techniques, though this isn't proven to be due to the robot alone and partly reflects the implant and the surgeon.⁷,⁸
What are the risks and trade-offs?
Robotic assistance doesn't remove the risks that come with any joint replacement, among them infection, blood clots, stiffness, and the small chance of further surgery. A few trade-offs are specific to the robotic approach. The operation takes a little longer, around 15 to 20 minutes more for knee replacement, and planning requires a CT scan, which involves a small amount of additional radiation. The robot supports the surgeon's judgement rather than replacing it. Whether robotic-assisted surgery suits your situation is discussed in detail at your consultation, and as with all joint replacement, individual results vary.
Common questions
What does robotic assistance actually change?
Robotic assistance is a planning and guidance tool, not an automated surgeon. Dr Tsung performs the operation and stays in control throughout. Before surgery, a CT scan of your joint is turned into a 3D model and the implant is planned onto it. During the operation the robotic arm helps him follow that plan precisely and keeps the instrument within the planned area. The robot does not move on its own.
Is robotic-assisted surgery more accurate than conventional surgery?
The best-proven benefit of robotic assistance is precision. Across hip and knee replacement, published studies show it places the implant within the planned position more consistently than manual technique, with fewer alignment outliers. What it has not been shown to do is make a joint replacement last longer or need fewer revisions than well-performed conventional surgery. Precision is the proven benefit; it is not a guarantee of a better long-term result, and individual results vary.
Does robotic-assisted surgery cost more for the patient?
No. Using a robotic-assisted system does not add to the cost of your surgery. Robotic planning is part of how Dr Tsung performs hip and knee replacement, not a paid extra. Your out-of-pocket cost depends on the procedure and your health fund, and we go through it with you before surgery. You'll find our fees and what your health fund covers on the fees and health funds page.
Is the Mako robot used for both hip and knee replacement?
Yes. Dr Tsung uses the Mako system for hip replacement, total knee replacement and partial (unicompartmental) knee replacement, and has done so since 2016. The benefit is a little different for each. In the hip it helps position the socket accurately, and in the knee it delivers the functional alignment plan. Partial knee replacement is less forgiving of small positioning errors, which is where precise planning may matter most.
Does robotic assistance make the operation take longer?
Robotic-assisted joint replacement takes a little longer than conventional surgery, but the difference is modest. Robotic-assisted hip replacement, total knee replacement and partial knee replacement take around 45 to 60 minutes on average. Planning also requires a CT scan a week or two beforehand, which involves a small amount of additional radiation. The robotic step does not remove the risks that come with any joint replacement, such as infection, blood clots and stiffness, and individual results vary.
Book or refer
To see Dr Tsung you’ll need a referral from your GP or another specialist. Call reception on (07) 5676 9930 to book your first appointment, or email hello@sgco.au. New patients can pre-register online before the visit; the form prepares your records and does not book an appointment. For costs, see fees and health funds.
References
- Ruangsomboon P, et al. Robotic-assisted versus conventional total knee arthroplasty: a meta-analysis of randomised controlled trials. Annals of Medicine and Surgery. 2025.
- Loke RWK, et al. MAKO robotic-assisted compared to conventional total hip arthroplasty for hip osteoarthritis: a systematic review and meta-analysis. Journal of Orthopaedic Surgery and Research. 2025;20:466.
- Hannon CP, et al. Does robotic assistance influence recovery after total knee arthroplasty? Bone & Joint Journal. 2025;107-B(10):1054–1063.
- Batailler C, et al. MAKO CT-based robotic arm-assisted system is a reliable procedure for total knee arthroplasty: a systematic review. Knee Surgery, Sports Traumatology, Arthroscopy. 2021;29:3585–3598.
- Sodhi K, et al. Robotic-assisted total knee arthroplasty with MAKO is associated with improved functional outcomes: a systematic review and meta-analysis. Bone & Joint Open. 2025;6(11):1382–1393.
- Clement ND, et al. Robotic arm-assisted versus manual total knee arthroplasty (ROAM): a randomised controlled trial. Bone & Joint Journal. 2024;106-B(5):450–459.
- Chen J, et al. Survivorship in robotic total knee arthroplasty compared with conventional total knee arthroplasty: a systematic review and meta-analysis. Arthroplasty. 2025;7:21.
- Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR). Hip, Knee & Shoulder Arthroplasty: 2025 Annual Report. Adelaide: AOA; 2025.
- Di Gangi C, et al. Robotic-assisted total hip arthroplasty and reduced dislocation risk. Journal of Arthroplasty. 2024;39(9S2):S359–S366.
- Sun C, et al. Comparison of MAKO robotic-assisted and manual unicompartmental knee arthroplasty: a meta-analysis of radiographic precision and short-term functional results. Journal of Robotic Surgery. 2026;20:307.